Pneumonia on X-Ray and What It Means
What Happens in the Lungs When Pneumonia Develops
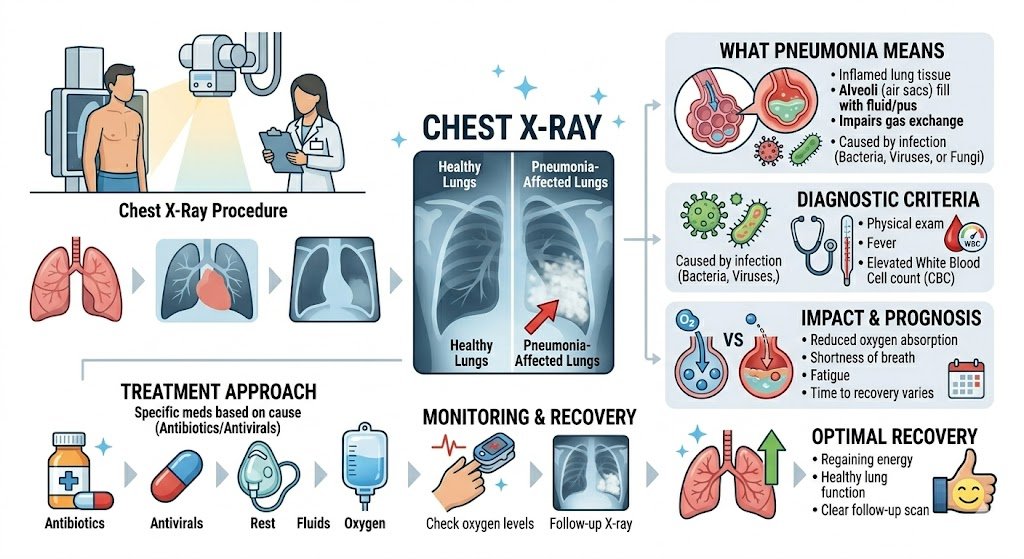
Pneumonia is not just a simple chest infection. It is a condition where the tiny air sacs inside your lungs, known as alveoli, fill up with fluid, pus, or other material instead of air. When that happens, the affected part of the lung stops doing its main job — which is to bring oxygen into the blood and push carbon dioxide out. The result is that the body starts working harder to breathe, oxygen levels in the blood can fall, and the person may feel short of breath, tired, and feverish all at once.
What makes pneumonia different from a regular cold or cough is that it reaches deep into the lung tissue itself. A regular chest cold or bronchitis mostly stays in the breathing tubes, called bronchi. But pneumonia goes further. It reaches the alveoli and causes them to become inflamed and filled with fluid. This is why a doctor will often order a chest X-ray it is the fastest and most widely available way to confirm whether pneumonia is truly present in the lung, and if so, where it is and how much of the lung is affected.
Understanding how X-rays show pneumonia is useful not just for doctors, but also for patients and families who want to know what the report actually means. Many people receive a radiology report and feel confused by the technical terms. This article explains all of that in straightforward language.
About how pneumonia starts:
A bacteria, virus, or fungus enters the lower respiratory tract
The immune system sends white blood cells to fight the infection
Fluid and cells collect in the alveoli, replacing air
The affected area becomes dense and stops letting air pass through
This density shows up on an X-ray as a white or grey patch
How a Chest X-Ray Works and Why It Shows Pneumonia
A chest X-ray uses a small amount of radiation that passes through the body and hits a detector or film on the other side. Different tissues block radiation in different amounts. Bone blocks a lot of radiation and shows up white. Air blocks almost none and shows up black. Soft tissue like heart muscle and blood vessels show up in shades of grey.
Healthy lungs are mostly filled with air, so they appear black or very dark on an X-ray. When part of a lung fills with fluid or pus because of pneumonia, that area stops being air-filled. It becomes denser. On the X-ray, that dense area appears whiter or greyer than the rest of the lung. Radiologists and doctors look for these white or grey patches when reading a chest X-ray for possible pneumonia.
This is why the standard chest X-ray remains the most commonly used first step in diagnosing pneumonia. It is quick, affordable, widely available, and gives a clear picture of which parts of the lung are affected.
| What is seen on X-ray | What it means |
| Dark (black) lung fields | Normal, air-filled lung |
| White or grey patch in lung | Fluid, pus, or collapse — could be pneumonia |
| Hazy shadow spreading across lung | Possible atypical or viral pneumonia |
| White area at lung base with flat top | Fluid around the lung (pleural effusion) |
| Complete whiteness of one lung | Severe consolidation or lung collapse |
It is important to know that not every white patch on a chest X-ray means pneumonia. Tumors, fluid around the lungs, and lung collapse can also look white. This is why a radiologist studies the shape, location, and pattern of the opacity carefully before deciding what it represents.
The Term “Consolidation” and What It Actually Looks Like
When doctors and radiologists see a dense white area in the lung on X-ray, they often call it consolidation. This word simply means that part of the lung has become solid instead of air-filled. In a healthy lung, the alveoli are tiny open sacs. In consolidation, those sacs fill up with fluid, pus, or inflammatory cells. The area stops being spongy and open, and it becomes dense, almost like a solid piece of tissue.
On an X-ray, consolidation appears as a clearly white or grey area within the lung field. The edges of this area may be sharp or blurry depending on the type of pneumonia and where in the lung it is located. One important feature that radiologists look for is called air bronchograms. This is when the white consolidated area has thin dark lines running through it — these dark lines are the air-filled breathing tubes (bronchi) that are still open and visible because the surrounding lung tissue has become dense. Seeing air bronchograms inside a white patch strongly suggests the cause is pneumonia or another inflammatory process, rather than a tumor or complete lung collapse.
A quote from Dr. Paul Stark, a chest radiologist, captures this well: “The presence of air bronchograms within an opacity almost always tells you that the airways remain patent while the alveolar spaces are filled that pattern speaks strongly for an airspace disease like pneumonia, not an obstructing mass.”
Features of consolidation on X-ray:
White or grey patch within the lung
May be well-defined or hazy at the edges
Can involve part of a lobe, a full lobe, or multiple lobes
Air bronchograms may be visible inside the white area
Usually stays within the boundary of one lobe in bacterial pneumonia
Lobar Pneumonia Versus Bronchopneumonia: Different Patterns on X-Ray
Not all pneumonia looks the same on an X-ray. One of the most important distinctions is between lobar pneumonia and bronchopneumonia. These two types have very different appearances on imaging, and recognizing the difference helps doctors understand what type of germ may be causing the infection.
Lobar pneumonia affects an entire lobe of the lung. Each lung has lobes — the right lung has three lobes and the left lung has two. When a bacteria like Streptococcus pneumoniae (pneumococcus) infects a person, it tends to spread through the alveoli in a wave-like fashion, filling up an entire lobe systematically. On an X-ray, this shows up as a solid, clearly defined white area that fills the space of one entire lobe.
Bronchopneumonia, by contrast, starts in the small breathing tubes (bronchioles) and spreads outward in patches. Instead of one solid white lobe, the X-ray shows multiple small, fluffy, or patchy white areas scattered through the lung. Bronchopneumonia is common in the elderly, in young children, and in people with weakened immune systems.
| Feature | Lobar Pneumonia | Bronchopneumonia |
| Pattern | Dense, solid white lobe | Patchy, scattered shadows |
| Distribution | Usually one lobe | Often bilateral, multiple areas |
| Edges | Fairly well-defined | Irregular, fluffy |
| Common cause | Streptococcus pneumoniae | Mixed bacteria, Staphylococcus |
| Common in | Healthy adults | Elderly, children, immunocompromised |
| Air bronchograms | Common | Less common |
A typical Pneumonia and How It Shows Up Differently
Some types of pneumonia are called atypical because they behave differently from classic bacterial pneumonia. They are caused by organisms like Mycoplasma pneumoniae, Chlamydophila pneumoniae, and Legionella pneumophila. They are also caused by many common viruses, including influenza, respiratory syncytial virus (RSV), and SARS-CoV-2, the virus responsible for COVID-19.
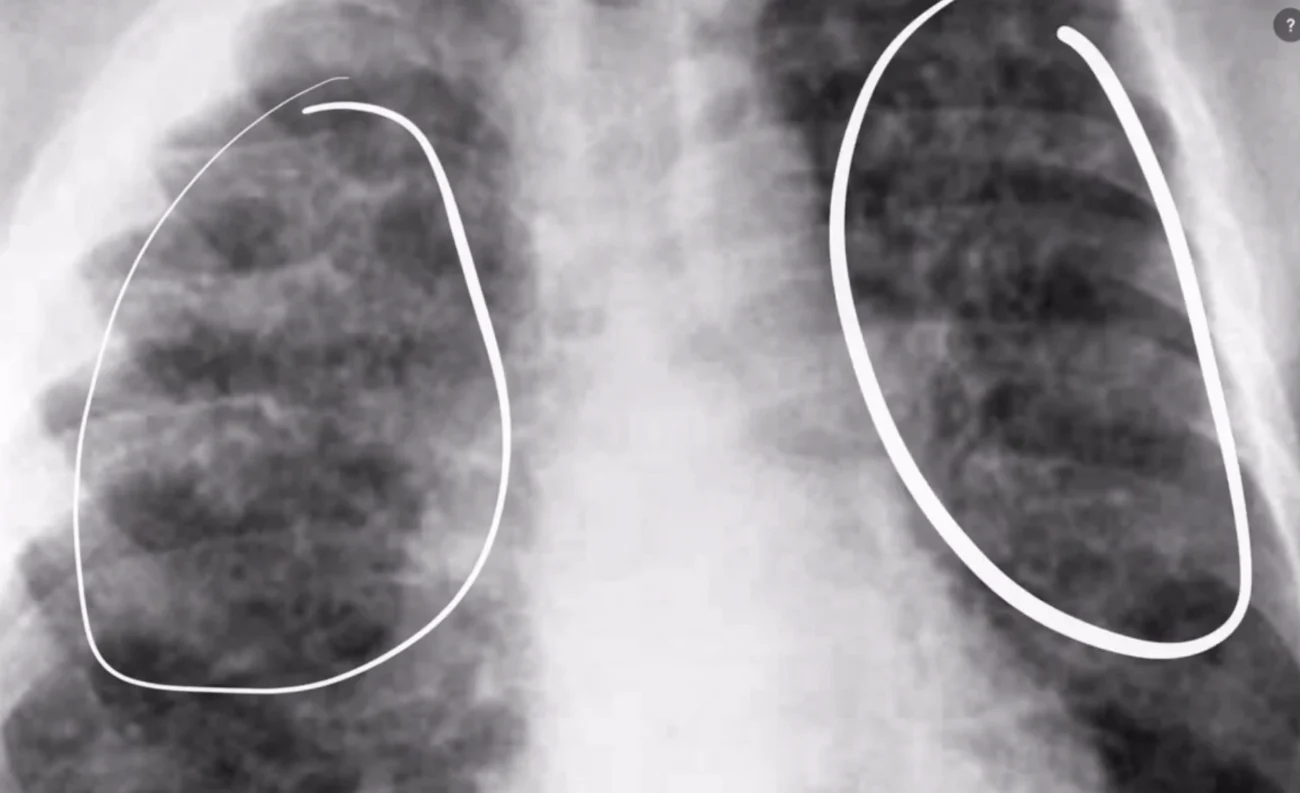
In atypical pneumonia, the infection does not just fill up the alveoli with pus and fluid. Instead, it causes inflammation mainly in the walls of the alveoli and in the tissue between the alveoli, which is called the interstitium. Because the inflammation is in the walls and tissue rather than filling the air sacs completely, the X-ray looks different.
Instead of a solid white consolidation, atypical pneumonia often produces a fine, hazy, or ground-glass appearance on the X-ray. The lung looks like it has a diffuse haziness or a slight whitening spread across a large area, rather than one solid white patch. During the COVID-19 pandemic, the characteristic X-ray appearance of COVID-19 pneumonia became one of the most recognized imaging patterns in radiology — typically showing bilateral, peripheral, and lower-zone predominant ground-glass opacities.
Appearances of atypical pneumonia on X-ray:
Diffuse haziness or ground-glass opacity
Bilateral involvement (both lungs affected)
Reticular (net-like) pattern from interstitial inflammation
Less well-defined than lobar consolidation
May look deceptively mild on X-ray even when the patient feels very ill
The Right Lower Lobe: Why Pneumonia Often Appears There
When people ask where pneumonia commonly shows up on a chest X-ray, the right lower lobe is one of the most frequent answers. This is not a coincidence. It relates to the anatomy of the airways. The right main bronchus, which is the large breathing tube that leads air into the right lung, is more vertical and wider than the left one. This means that if you breathe in something — like bacteria-containing droplets or aspirated food particles it is more likely to travel down the right bronchus and settle in the lower part of the right lung.
The lower lobes of both lungs are also areas where secretions tend to pool when a person is lying in bed, which is why hospital-acquired pneumonia in bedridden patients often shows up at the bases of the lungs. On an X-ray, pneumonia in the right lower lobe appears as a white density at the right base of the lung. Sometimes it can be partly hidden behind the shadow of the heart.
| Location | Common risk factor |
| Right lower lobe | Aspiration, anatomy of right bronchus |
| Left lower lobe | Bedridden patients, post-surgical |
| Right upper lobe | Tuberculosis reactivation in adults |
| Both lower lobes | Viral pneumonia, aspiration |
| Bilateral diffuse | Severe infection, immunocompromised patients |
Round Pneumonia: An Unusual Appearance That Confuses People
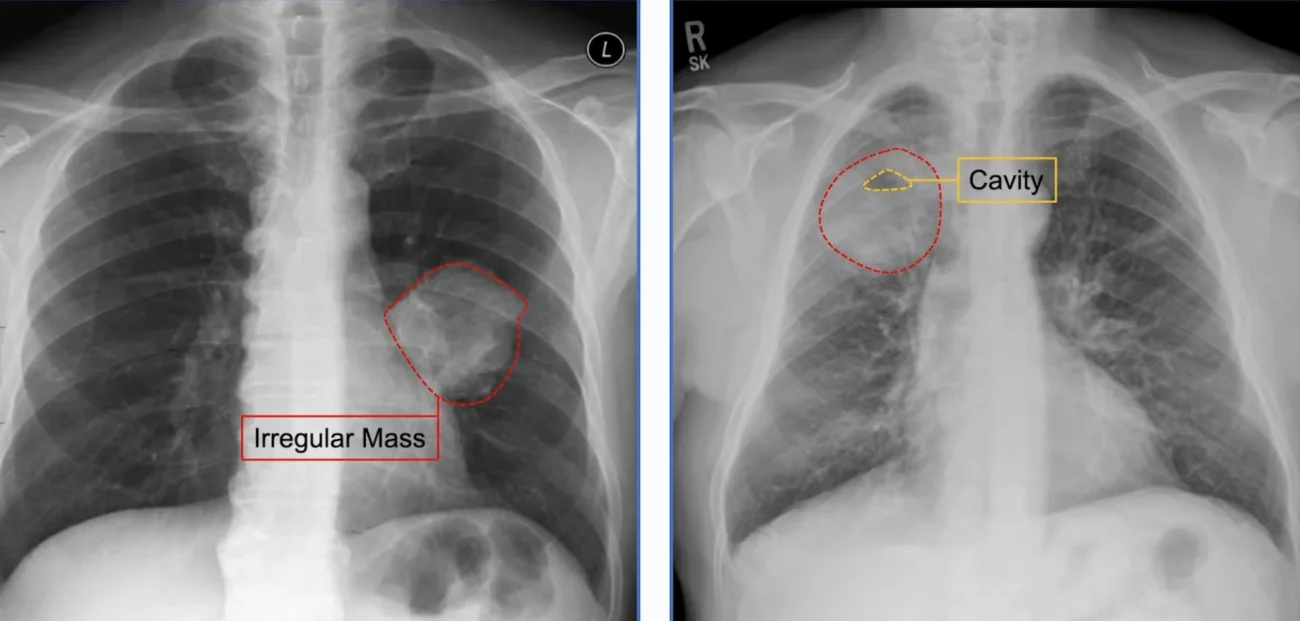
Most people expect pneumonia to look like an irregular or spreading patch on an X-ray. But there is a type called round pneumonia that appears as a round or oval white mass in the lung. This can easily be mistaken for a lung tumor, and it causes a lot of anxiety for patients and their families when the radiologist describes a round opacity.
Round pneumonia is more common in children than in adults, and it is most often caused by Streptococcus pneumoniae.
The reason it forms a round shape relates to the anatomy of the lung in younger patients the connections between alveoli (called pores of Kohn) are less developed in children, so infection spreads in a more circular pattern.
What helps doctors tell round pneumonia apart from a lung tumor on X-ray is the clinical picture. A child or adult who is feverish, coughing, and has an elevated white cell count in the blood is much more likely to have round pneumonia than a tumor. Round pneumonia also responds to antibiotics within 7–10 days, whereas a tumor would stay or grow.
Features that help distinguish round pneumonia from a tumor:
Age (more common in children)
Fever and acute onset of symptoms
Elevated infection markers in blood
Responds to antibiotics within 7–10 days
Follow-up X-ray shows resolution (clearing)
Pleural Effusion Alongside Pneumonia: What It Means
Sometimes when looking at a chest X-ray for pneumonia, the radiologist also notices fluid around the lung. This fluid, which collects in the space between the lung and the chest wall, is called a pleural effusion. It is a complication that can develop in pneumonia, and seeing it on an X-ray is an important finding that changes how the patient is managed.
On a chest X-ray, a pleural effusion appears as a white density at the bottom of the lung, often with a curved upper border (called a meniscus sign). Small effusions may only cause blunting of the costophrenic angle, which is the sharp corner where the lung meets the diaphragm.
When a pleural effusion develops alongside pneumonia, doctors want to know whether the fluid is a simple reactive effusion or whether it is an infected effusion called an empyema. An empyema is when the fluid itself becomes infected and turns into pus — a more serious complication that may require draining with a needle or tube.
Signs of pleural effusion on chest X-ray:
Blunting of the costophrenic angle (the sharp lower corner of the lung)
White density at the base of the chest with a curved upper border
Shifting of the mediastinum away from the effusion (in large effusions)
Loss of visibility of the diaphragm outline on that side
How Doctors Rate the Severity of Pneumonia Using X-Ray Findings
Looking at a chest X-ray is one part of assessing how serious a case of pneumonia is, but it is not the only tool. Doctors use scoring systems that combine clinical signs, blood test results, and X-ray findings together to decide how sick a patient is and whether they need to be treated in hospital or can be managed at home.
One commonly used scoring system in adults is the CURB-65 score. It gives points for confusion, raised blood urea, fast breathing, low blood pressure, and age over 65. The X-ray finding of more than one lobe being involved (multilobar pneumonia) is often taken as an additional sign of severity.
On the X-ray itself, features that suggest a more severe case include:
Involvement of more than one lobe
Bilateral pneumonia (both lungs affected)
Cavitation within the consolidated area
Large pleural effusion
Rapidly expanding consolidation on repeat X-rays taken hours apart
Cavitation Inside Pneumonia: A Sign That Should Not Be Ignored
Some types of pneumonia can form a cavity inside the consolidated area of the lung. On an X-ray, this appears as a white patch (the consolidation) with a dark area inside it — sometimes with a visible fluid level, indicating the cavity contains both liquid and air. This is called a cavitating pneumonia or lung abscess.
Cavitation in pneumonia almost always suggests a more serious or aggressive infection. A lung abscess is when a necrotic (dying) area within the pneumonia forms a pocket of pus that becomes walled off. It looks like a round, thick-walled cavity on X-ray, often with an air-fluid level. The treatment is prolonged antibiotic therapy, and sometimes drainage or surgery is needed.
| Organism | Common location of cavity | Typical patient |
| Tuberculosis | Upper lobe | Contacts of TB cases, immigrants from endemic areas |
| Staphylococcus aureus | Any lobe | Post-influenza, intravenous drug users |
| Klebsiella pneumoniae | Upper lobe | Alcoholics, diabetics |
| Anaerobic bacteria | Lower lobe | Aspiration, poor dental hygiene |
| Fungal (Aspergillus) | Any, often upper | Immunocompromised, cancer patients |
What a Normal Chest X-Ray Means When Pneumonia Is Suspected
A very important point that confuses many patients is this: a normal chest X-ray does not always rule out pneumonia. There are situations where a person has all the symptoms of pneumonia — fever, cough, difficulty breathing — but the chest X-ray looks normal or near-normal.
In the very early stages of pneumonia, the consolidation may not yet be dense enough to show clearly on an X-ray. In people who are dehydrated, the fluid that fills the alveoli may be reduced — once the patient is given fluids, the pneumonia can actually become more visible on a repeat X-ray taken a day or two later. Some areas of the lung are also harder to see on a standard frontal X-ray.
When clinical suspicion is high but the X-ray is normal, doctors may:
Treat empirically — start antibiotics based on clinical judgment without waiting for imaging confirmation
Order a CT scan of the chest, which is far more sensitive than plain X-ray
Repeat the chest X-ray after 24–48 hours
Order additional blood tests to look for markers of infection
Using CT Scans When the Chest X-Ray Is Not Enough
CT scanning is a much more detailed form of imaging that can detect pneumonia earlier and with more precision than a plain X-ray. On a CT scan, early pneumonia shows up as ground-glass opacity — a hazy increase in density that still allows the underlying lung structure to be visible. CT can also detect small areas of consolidation, pleural effusion, lymph node enlargement, and cavitation that are not visible on plain films.
CT scanning is typically reserved for cases where the X-ray is normal but clinical suspicion is high, where findings are ambiguous and a tumor cannot be excluded, where the patient is not responding to treatment as expected, where a complication such as abscess or empyema is suspected, or where the patient is immunocompromised and the cause of infection is unclear.
What Happens to the X-Ray as Pneumonia Improves with Treatment
When pneumonia is treated with the right antibiotics or antiviral medications, the patient usually starts to feel better within 48 to 72 hours. However, the chest X-ray does not clear up as fast as the patient feels better. This is a very important point that patients and families need to understand.
Radiological clearing — meaning the white patch on the X-ray getting smaller and eventually disappearing — takes longer than clinical improvement. In uncomplicated pneumonia in a healthy young adult, the X-ray may not fully clear for 4 to 6 weeks. In elderly patients or those with other health problems, it can take much longer, sometimes 3 months or more.
| Time after treatment starts | Expected X-ray findings |
| 24–72 hours | No change or even apparent worsening |
| 1–2 weeks | Gradual reduction in size of consolidation |
| 3–4 weeks | Significant improvement; consolidation much smaller |
| 4–8 weeks | Full or near-full clearance in most healthy adults |
| 8–12 weeks | Full clearance in elderly or those with other conditions |
Pneumonia Versus Other White Patches on a Chest X-Ray
One of the most challenging parts of interpreting a chest X-ray is distinguishing pneumonia from other conditions that also produce white patches in the lung. Conditions that can look similar include lung cancer, pulmonary edema, pulmonary embolism with infarction, lung collapse (atelectasis), and eosinophilic pneumonia.
| Condition | Key distinguishing X-ray features |
| Pneumonia | Consolidation with air bronchograms, clinical fever |
| Heart failure / pulmonary edema | Bilateral hazy shadows, enlarged heart, fluid in fissures |
| Lung cancer | Well-defined mass, no fever, no resolution with antibiotics |
| Lung collapse | Volume loss, trachea and mediastinum shift toward opacity |
| Pleural effusion | White opacity at base with curved upper border |
Pneumonia in Children: Why the X-Ray Looks Different
Chest X-rays in children with pneumonia can look different from those in adults. Children, especially young ones, are more prone to viral pneumonia, which tends to produce the hazy, bilateral, interstitial pattern rather than the solid lobar consolidation more common in adults.
In infants, the thymus gland — which sits in the front of the chest — is prominent and appears as a sail-shaped or triangular white area in the upper chest. This is completely normal, but it can be mistaken for pneumonia by someone not familiar with pediatric X-rays. Viral pneumonia in children often shows a pattern called peribronchial thickening — the walls of the breathing tubes appear thickened, giving a tramline or ring shadow appearance.
Features specific to pediatric chest X-ray interpretation:
Prominent thymus in infants (normal, should not be mistaken for disease)
Round pneumonia more common than in adults
Viral pneumonia more common overall, producing interstitial or peribronchial patterns
Bilateral haziness common in RSV pneumonia
Rapid resolution once treatment is started in most uncomplicated cases
Special Populations: Immunocompromised Patients and Their Unique X-Ray Patterns
Patients whose immune systems are weakened by HIV/AIDS, cancer chemotherapy, organ transplantation, or long-term steroid use can develop pneumonia from organisms that would not cause illness in a healthy person. These are called opportunistic infections, and they often produce unusual X-ray patterns.
Pneumocystis jirovecii pneumonia (formerly called PCP) is one of the most important opportunistic infections, seen mainly in HIV-positive patients with low CD4 counts. On chest X-ray, it typically produces bilateral, diffuse, fine granular or ground-glass haziness spreading from the hilum outward. In early stages, the X-ray can look surprisingly normal despite the patient being very breathless.
Invasive fungal infections like Aspergillus can produce nodular shadows, a halo sign on CT, or cavities. These unusual patterns are important clues for doctors to look for fungal or atypical infections rather than just treating with standard bacterial pneumonia antibiotics.
Tuberculosis and How It Differs from Standard Pneumonia on X-Ray
Tuberculosis (TB) deserves special mention because it is a disease that primarily affects the lungs and can look like many different things on a chest X-ray. TB is caused by Mycobacterium tuberculosis and remains one of the leading infectious causes of death worldwide.
Primary TB in children and young adults often shows a small consolidation anywhere in the lung, combined with enlarged lymph nodes at the hilum — a combination called a primary complex or Ghon complex. Reactivation TB in adults typically shows upper lobe cavities, fibrosis, and calcified nodules. Miliary TB, the most dramatic form, shows innumerable tiny white dots distributed evenly throughout both lungs, resembling millet seeds.
| TB type | X-ray appearance | Who is commonly affected |
| Primary TB | Small consolidation + hilar lymph nodes | Children, new exposures |
| Reactivation TB | Upper lobe cavities, fibrosis | Adults with old TB exposure |
| Miliary TB | Diffuse tiny nodules throughout both lungs | Immunocompromised, very young |
| TB pleural effusion | Unilateral pleural effusion | Young adults, primary infection |
What Patients Should Ask Their Doctor After a Chest X-Ray
When a patient is told they have pneumonia on their X-ray, it can feel frightening and confusing. Understanding what the findings mean and what to expect can reduce anxiety and help patients take an active role in their own recovery.
Practical questions a patient can ask after receiving a pneumonia diagnosis:
Which lobe or lobes of my lung are affected?
How serious does the X-ray look — is one lobe involved or more?
Is there any fluid around my lungs?
Is there any sign of a cavity or abscess?
What type of pneumonia do you think this is — bacterial, viral, or atypical?
Do I need to be admitted to hospital or can I be treated at home?
When should I come back for a follow-up X-ray?
At what point should I be worried if my X-ray has not cleared?
When Pneumonia Leaves Scars: Residual Changes After Recovery
Most cases of pneumonia clear up completely without leaving any permanent damage. However, in some cases — especially severe pneumonia, delayed treatment, certain organisms, or repeated infections — permanent changes can be left behind on the X-ray even after the person has fully recovered.
These permanent changes can include fibrosis (scarring appearing as irregular white lines), bronchiectasis (permanent widening and scarring of the bronchi showing as tramline shadows), calcified lymph nodes (bright white spots from old TB or fungal infection), and pleural thickening (a white rind along the edge of the lung after a pleural effusion).
Understanding that these residual changes may be present on future X-rays is important. A patient who has had pneumonia may have a chest X-ray for a different reason years later, and the radiologist may comment on these old changes. This can cause unnecessary worry unless the treating doctor explains that these are old, healed changes and not a new infection.
Preventing Pneumonia and the Role of Regular Chest Monitoring
Prevention is always better than treatment, and there are several proven ways to reduce the risk of pneumonia, particularly for people who are at higher risk. Vaccines play a major role. The pneumococcal vaccine protects against Streptococcus pneumoniae and is recommended for adults over 65, younger adults with chronic health conditions, and children. The influenza vaccine reduces the risk of flu-related pneumonia.
Beyond vaccination, the following steps reduce pneumonia risk:
Not smoking — smoking damages the cilia that line the airways and help sweep out debris and germs
Treating chronic conditions like asthma, diabetes, and heart failure well
Practicing good hand hygiene, especially during cold and flu season
Seeking early medical attention when a chest infection does not improve after a few days
For people in hospital or on bed rest, regular position changes and breathing exercises to prevent aspiration pneumonia
Reading the Radiology Report: A Plain-English Guide to Common Terms
When a chest X-ray is taken, a radiologist reads it and writes a formal report. Patients often request a copy of this report and find it full of unfamiliar medical terms. Here is a straightforward explanation of terms commonly found in pneumonia reports.
| Report term | Plain-language meaning |
| Consolidation | Part of the lung has become solid with fluid or pus |
| Ground-glass opacity | Hazy whitening; typical of viral or atypical pneumonia |
| Air bronchograms | Airways visible inside the white patch; suggests pneumonia |
| Pleural effusion | Fluid around the lung |
| Atelectasis | A section of lung has collapsed |
| Cavitation | A hole or hollow space inside the lung tissue |
| Bilateral | Both lungs affected |
| Reticular pattern | Net-like shadows; inflamed tissue walls |
| No acute cardiopulmonary abnormality | Nothing wrong found with the heart or lungs |
Final Thoughts: Putting the Chest X-Ray in Context
A chest X-ray is a powerful but imperfect tool. It can confirm pneumonia, suggest its type and severity, detect complications, and track recovery. But it does not tell the whole story on its own. The findings on the X-ray must always be read alongside the patient’s symptoms, physical examination, blood test results, and medical history.
A small white patch in the lung of a young healthy person with two days of fever and a productive cough almost certainly represents bacterial pneumonia. The same white patch in a 70-year-old smoker who has been coughing for three months might need further investigation to rule out cancer. Context is everything.
For patients, understanding what a chest X-ray shows in pneumonia takes away some of the fear that comes with an uncertain diagnosis. Knowing that a dense white patch means consolidated lung, that air bronchograms suggest infection rather than tumor, that the X-ray often lags behind clinical recovery, and that most pneumonia heals without permanent damage — all of this helps patients engage more meaningfully with their doctors and their own recovery.
Pneumonia is treatable. With the right diagnosis, correct antibiotics or antiviral treatment, appropriate supportive care, and close follow-up, the vast majority of people recover completely. The chest X-ray is one of the most important guides along that recovery journey.
